What Is Dizziness & Vertigo
Dizziness and vertigo symptoms can range from the merely uncomfortable to the incapacitating. Severe vertigo can limit life activities and cause nausea, headaches, abnormal eye movements, and imbalance.

Hearing loss is defined as one of three types:
Aging and chronic exposure to loud noises both contribute to hearing loss. Other factors, such as excessive earwax, can temporarily reduce how well your ears conduct sounds.
You can’t reverse most types of hearing loss. However, you and your doctor or a hearing specialist can take steps to improve what you hear.
Signs and symptoms of hearing loss may include:
To understand how hearing loss occurs, it can be helpful to first understand how you hear.
How you hear
Your ear consists of three major areas: outer ear, middle ear and inner ear. Sound waves pass through the outer ear and cause vibrations at the eardrum. The eardrum and three small bones of the middle ear amplify the vibrations as they travel to the inner ear. There, the vibrations pass through fluid in a snail-shaped structure in the inner ear (cochlea).
Attached to nerve cells in the cochlea are thousands of tiny hairs that help translate sound vibrations into electrical signals that are transmitted to your brain. Your brain turns these signals into sound.
How hearing loss can occur
Causes of hearing loss include:

Factors that may damage or lead to loss of the hairs and nerve cells in your inner ear include:
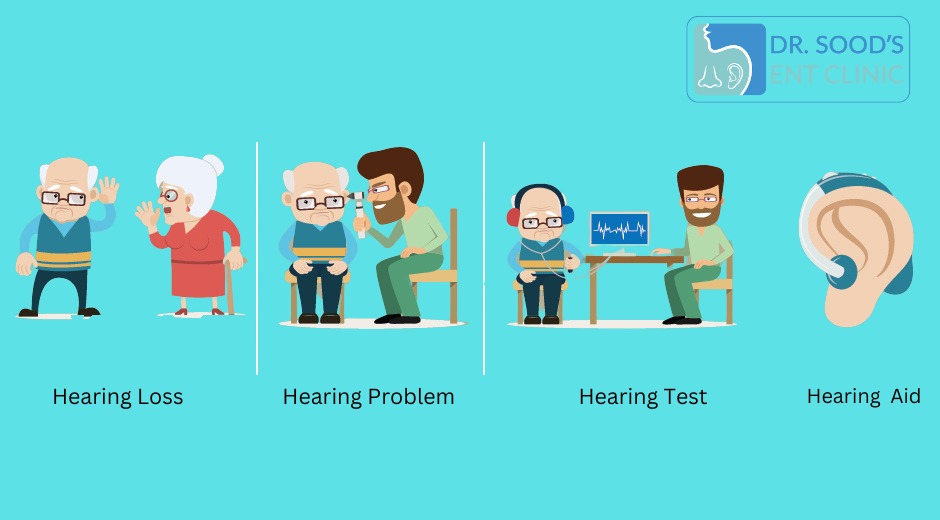
Patients who suspect something is wrong with their hearing will initially go and see their doctor.
The doctor will talk to the patient and ask several questions regarding the symptoms, including when they started, whether or not they have gotten worse, and whether the individual is feeling pain alongside the hearing loss.
The doctor will look into the ear using an otoscope. This is an instrument with a light at the end. The following may be detected during the examination:
The doctor will ask questions about the person’s experiences with hearing, including:
If you answered “yes” to most of the above questions, see a doctor and have your hearing checked.
A doctor may ask the patient to cover one ear and describe how well they hear words spoken at different volumes, as well as checking sensitivity to other sounds.
If the doctor suspects a hearing problem, they will probably be referred to either an ear, nose, and throat (ENT) specialist or an audiologist.
Further tests will be carried out, including:
A tuning fork test: This is also known as the Rinne test. A tuning fork is a metal instrument with two prongs that produces a sound when it is struck. Simple tuning fork tests may help the doctor detect whether there is any hearing loss, and where the problem is.
A tuning fork is vibrated and placed against the mastoid bone behind the ear. The patient is asked to indicate when they no longer hear any sound. The fork, which is still vibrating, is then placed 1 to 2 centimeters (cm) from the auditory canal. The patient is asked again whether they can hear the fork.
As air conduction is greater than bone conduction, the patient should be able to hear the vibration. If they cannot hear it at this point, it means that their bone conduction is superior to their air conduction.
This suggests a problem with sound waves getting to the cochlea through the ear canal.
Audiometer test: The patient wears earphones, and sounds are directed into one ear at a time. A range of sounds is presented to the patient at various tones. The patient has to signal each time a sound is heard.
Each tone is presented at various volumes, so that the audiologist can determine at which point the sound at that tone is no longer detected. The same test is carried out with words. The audiologist presents words at various tones and decibel levels to determine where the ability to hear stops.
Bone oscillator test: This is used to find out how well vibrations pass through the ossicles. A bone oscillator is placed against the mastoid. The aim is to gauge the function of the nerve that carries these signals to the brain.
The American Academy of Pediatrics (AAP) recommends that children have their hearing tests at the following times:
Help is available for people with all types of hearing loss. Treatment depends on both the cause and severity of the deafness.
Sensorineural hearing loss is incurable. When the hair cells in the cochlea are damaged, they cannot be repaired. However, various treatments and strategies can help improve quality of life.

“Epistaxis” is the medical term for a nosebleed. A nosebleed, meaning a loss of blood from the tissue that lines the inside of your nose, can occur in one or both nostrils. Usually, it only affects one nostril.
Epistaxis is common. About 60% of people will have at least one nosebleed in their lifetime. Only about 10% of cases are severe enough to require medical treatment.
Anyone can get nasal bleeding. Most people will have at least one case in their lifetime. However, some people are more likely to have a nosebleed. They include:
There are two main types of nosebleeds.
An anterior nosebleed starts in the front of your nose on the lower part of the wall that separates the two sides of your nose (septum). Capillaries and small blood vessels in this front area of your nose are fragile and can easily break and bleed. This is the most common type of epistaxis and usually isn’t serious. These nosebleeds are more common in children. You can usually treat these nosebleeds at home.
A posterior nosebleed occurs deep inside your nose. A bleed in larger blood vessels in the back part of your nose near your throat causes this type. It can result in heavy bleeding, which may flow down the back of your throat. You may need medical attention right away for this type of nosebleed. This type is more common in adults.
A nosebleed, or epistaxis, is the loss of blood from the tissue that lines the inside of your nose.
Most often, you won’t have any symptoms other than blood coming from your nose. If you have a posterior nosebleed, some blood may drain down the back of your throat into your stomach. This can cause a bad taste in the back of your throat and make you feel nauseated.
If you have additional symptoms, it may be a sign of a medical condition.
Most nosebleeds only affect one nostril, but they can affect both at the same time. Epistaxis has many causes. Fortunately, most aren’t serious.
The most common cause of nosebleeds is dry air. Hot, low-humidity climates or heated indoor air cause dry air. Both environments cause your nasal membrane (the delicate tissue inside your nose) to dry out and become crusty or cracked. This makes it more likely to bleed when rubbed or picked or when blowing your nose. You may also experience epistaxis after inserting an object in your nose or injuring your nose and/or face.
Other nosebleed causes may include:
Other less common causes of nosebleeds include:
A doctor will ask you questions about your nosebleed, including:
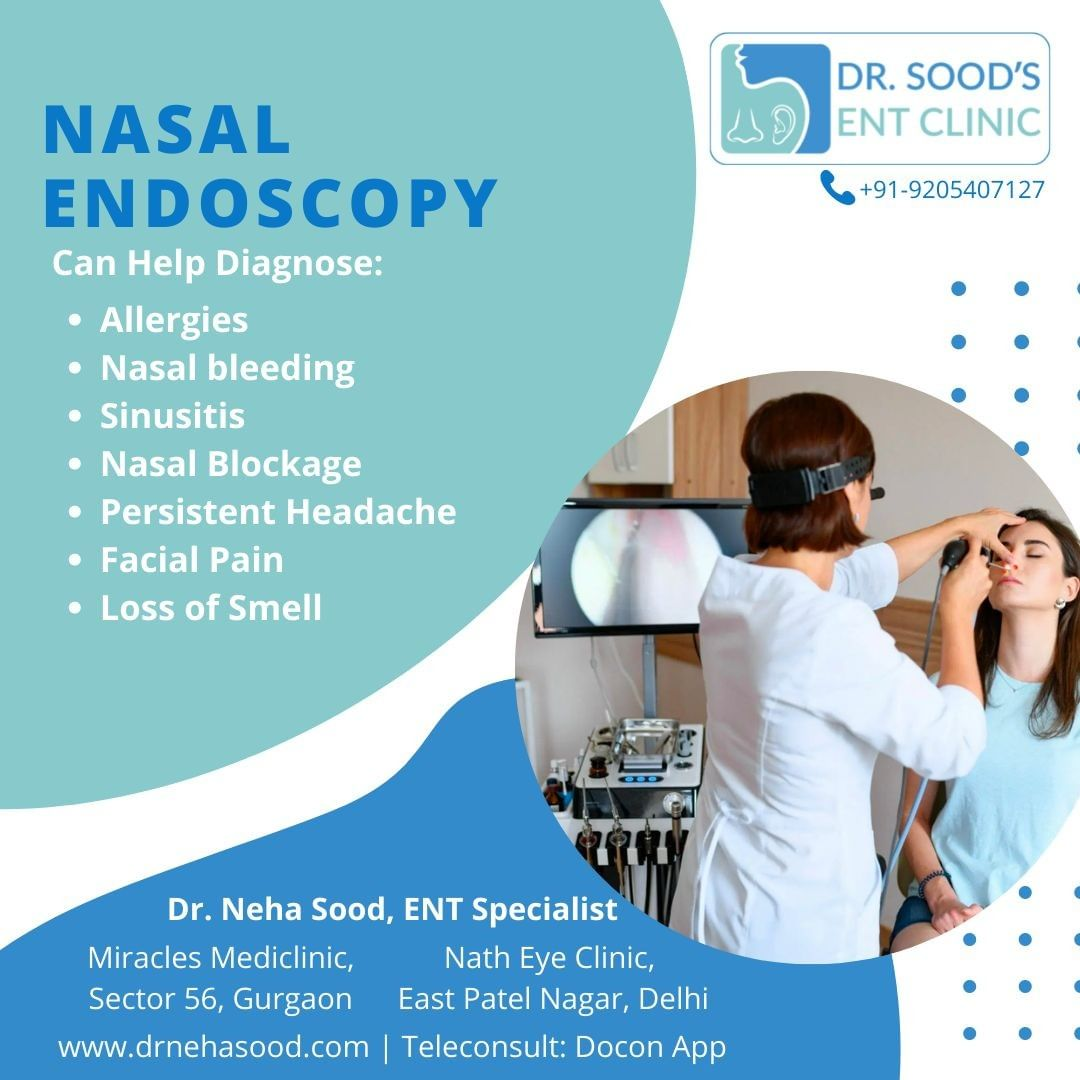
Next, your provider will examine your nose to determine the source of the bleeding and what may have caused it. They’ll use a small speculum to hold your nostril open and use various light sources or an endoscope (lighted scope) to see inside your nasal passages.
Your provider may use topical medications to numb (anesthetize) the lining of your nose and to narrow blood vessels. Your provider may remove clots and crusts from inside your nose. This can be unpleasant but isn’t painful.
Occasionally, they may order X-rays, a CT scan or blood tests to check for bleeding disorders, blood vessel abnormalities or nasal tumors.
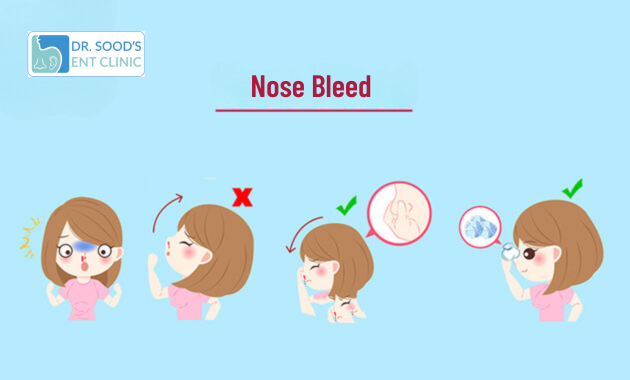
Use the following steps to stop a nosebleed at home.
Nosebleed treatment depends on the cause of the bleeding. Epistaxis treatment may include:
If you have any questions or concerns, don’t hesitate to call your doctor.
Although seeing blood coming out of your nose can be alarming, most nosebleeds aren’t serious. You can usually manage them at home. However, you should have some cases of epistaxis checked by a doctor. For instance, if you have frequent nosebleeds, see a provider. This could be an early sign of another medical issue that they’ll want to look into.
Some nosebleeds can start in the back of your nose. These cases of epistaxis usually involve large blood vessels resulting in heavy bleeding and can be dangerous. You’ll need medical attention for this type of bleed, especially if the bleeding occurs after an injury and the bleeding hasn’t stopped after 20 minutes of applying direct pressure to your nose.
Nosebleeds that occur higher on your septum or deeper in your nose may be harder to control. However, nosebleeds are rarely fatal. They account for 4 out of every 2.4 million deaths in the United States.
There are many non-serious reasons you may be getting frequent nosebleeds. They can affect one or both nostrils. The most common causes are:
The reasons for nosebleeds during sleep are the same as the reasons why they occur during the daytime — dried nasal membranes caused by dry air, allergies and upper respiratory infections that damage the delicate nasal membrane lining your nose. Sleeping with your head to the side may also put direct pressure on your nasal cavity and may be another reason for epistaxis at night.
Yes, you should drink plenty of fluids after a nosebleed. Good options include water, juice and other non-caffeinated liquids. After you experience epistaxis, some blood may drain down the back of your throat into your stomach. This may give you a bad taste in the back of your throat or make you feel nauseated. But drinking water won’t affect a nosebleed.
Call your doctor immediately, have someone drive you to the nearest emergency room or call 911 if:
Yes. Blood clots are clumps of blood that form in reaction to an injured blood vessel. Blood clotting prevents excessive bleeding when a blood vessel is damaged. When you pinch your nose to stop a nosebleed, the blood will begin to clot. It’ll normally remain there until you remove it or gently blow your nose.
Many factors can lead to headaches and nosebleeds. A common cause of both symptoms is a deviated septum (a shifted wall in your nose). One study found that epistaxis may be a precursor to migraines. Other common causes of headaches and nosebleeds may include: